
The Case for Indie Drugs
The uncomfortable truth about our Ozempic obsession

Everyone's hunting for the next Ozempic, the billion-dollar blockbuster that will treat millions of patients and generate massive returns. It's not that biopharma leaders don't see the appeal of smaller, more targeted treatments — they absolutely do.
The problem is they don't think the economics work.
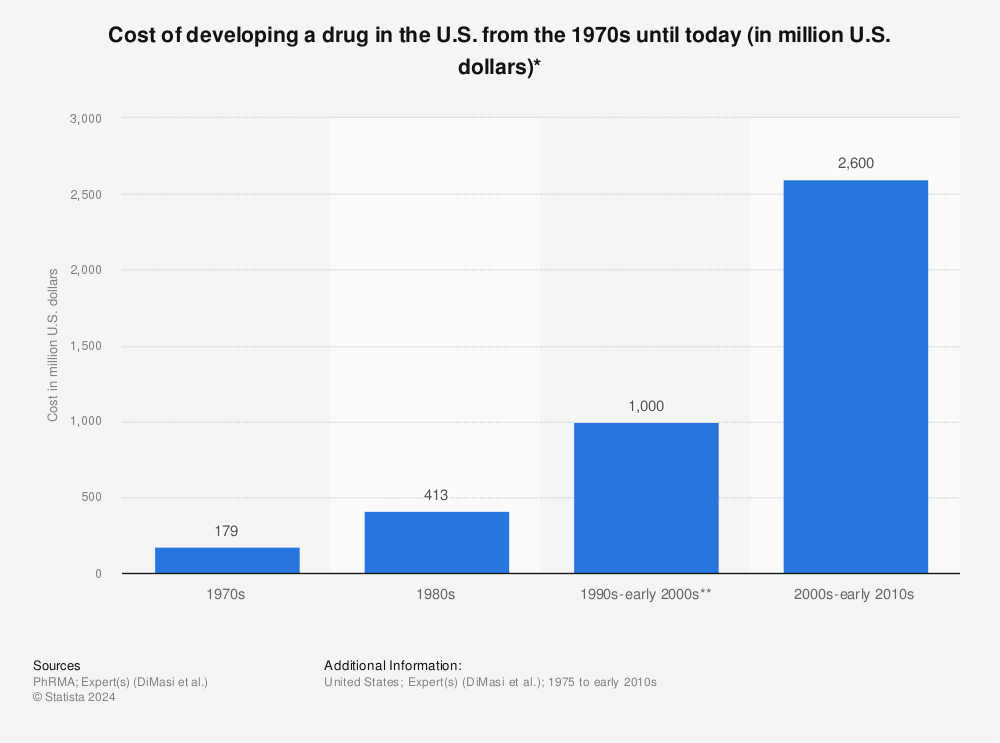
Why spend $2.6 billion developing a drug for 50,000 patients when you could spend the same amount targeting 50 million?
But what if the economics have to work? What if the biological reality of human disease is pushing us toward a future where personalized medicine demands not just better diagnostics, but a cornucopia of targeted drugs—and we need to solve the infrastructure to make it viable?
That question is a lot less sexy than imagining the next Ozempic, but looking at the data I find it much more likely to be the question we need to ask and answer if we really want to build a healthier future.
An Uncomfortable Reality
We should not be happy — at all — with the current state of the biopharma industry. The number of new drugs approved annually has barely grown since the 1970s despite the fact that in the 70s DNA sequencing didn't exist.

Meanwhile, the cost of bringing drugs to market has been rising rapidly, even relative to inflation. This means new treatments must either be more expensive, serve larger patient populations, or both.
At the same time, our understanding of disease biology has exploded. We now know that what we call "breast cancer" or "Alzheimer's" are actually dozens of distinct diseases with different molecular drivers.
The mismatch is stark: our awareness of biological complexity is expanding exponentially while our therapeutic output remains essentially flat.
The Promise of Personalization
The data is unambiguous. When treatments are properly matched to specific disease subtypes, response rates can jump dramatically. Recent research on ultra-rare tumor subtypes shows that matched therapy can yield clinical benefit rates of 85% compared to standard approaches.
Even our most advanced "personalized" treatments like CAR-T therapies — which customize treatment using each patient's own immune cells — still follow the blockbuster model at their core. They're one standardized approach applied broadly, just with individualized manufacturing. While impressive and exciting, it is unlikely they alone can get us to the degree of personalized medicine we know we want.
And it's not just about optimizing existing diseases. There are thousands of rare diseases affecting millions of patients worldwide, most with no approved treatments. These aren't edge cases—they represent a massive unmet medical need that the blockbuster model systematically ignores.
The Discovery Revolution
The technology for drug discovery has never been better. AI is creating a step change in our ability to model complex biological systems, predict drug interactions, and design precise therapies for niche patient populations. We can increasingly identify promising targets and compounds faster than ever before.
The tools for precision medicine are advancing rapidly. And the net outcome will hopefully be that we have 100 or 1000X drug candidates in the pipeline at any given time. Rare diseases will have pipelines like oncology does today, and oncology will be as big and diverse as the entire current landscape. That will be amazing, but the problem we’ll run into very quickly is that the real bottleneck isn't discovery — it's everything that comes after.
The Operational Bottleneck
Here's the uncomfortable truth: most of the $2.6 billion cost of bringing a drug to market isn't spent on discovery. It's spent on everything downstream—clinical trials, regulatory submissions, manufacturing setup, distribution networks, and countless other operational tasks.
And most of this work is still done by humans, manually. Teams of people analyzing clinical data, preparing regulatory documents, coordinating manufacturing processes, managing supply chains. The pharmaceutical industry may be high-tech in the lab, but it's remarkably analog in operations.
I suppose given the current climate it also has to be said that simply removing the regulatory hurdles is not going to give us the future we want, either. While it’s a noble cause for the government to work on and there is a real need to clear out sclerotic processes, we need better science and more coordination, not less of it.
This is where the real opportunity lies. Not in magically predicting the next Ozempic or ripping out the rigorous process of determining safety and efficacy, but in creating AI agents that can replace human work and help us bring drugs to market 10X more efficiently.
Employing a Billion Agents
When it comes to the business of biopharma, there's a far bigger opportunity to “hire” an army of agents to work alongside humans than to remove the humans entirely. For one thing, the humans that do this work are typically highly trained scientists with PhDs and a decade of experience. But more importantly, the number of people in these roles is nowhere near where it should be.
Think from first principles: given the cost of any misstep, a mid-sized biotech should employ dozens of analysts and BD people to monitor the landscape, look for opportunities, and coordinate partnerships for each asset in their pipeline. What you actually find is one or two people doing that work across an entire portfolio of assets.
Creating those teams of agents and enabling them to work autonomously will take time, but we need to work backwards from that place of abundance. We should be approving hundreds of drugs per year. There should be tens of thousands of drugs in the clinical pipeline and hundreds of thousands or millions of drugs in discovery. There should be teams of people working on every one of those assets, coordinating with each other across the industry and with governments to drive the cooperation and partnerships that make the whole thing flow.
That's where we need to be aiming with AI.